
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | /ælˈpræzəlæm/ or /ælˈpreɪzəlæm/ |
| Trade names | Xanax, Xanor, Niravam, others |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a684001 |
| License data |
|
| Pregnancy category |
|
| Dependence liability |
Very high |
| Addiction liability |
Moderate - high |
| Routes of administration |
By mouth |
| Drug class | Benzodiazepine |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 80–90% |
| Protein binding | 80% |
| Metabolism | Liver, via cytochrome P450 3A4 |
| Metabolites | Alpha-hydroxyalprazolam, 4-hydroxyalprazolam, beta-hydroxyalprazolam |
| Onset of action | 20~60 minutes |
| Elimination half-life | Full release: 11~13 hours Extended release: 11~16 hours |
| Duration of action | Full release: 6 hours Extended release: 11.3 hours |
| Excretion | Kidney |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.044.849 |
| Chemical and physical data | |
| Formula | C17H13ClN4 |
| Molar mass | 308.77 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
| (verify) | |
Alprazolam, sold under the brand name Xanax, among others, is a fast-acting, potent tranquilizer of moderate duration within the triazolobenzodiazepine group of chemicals called benzodiazepines. Alprazolam is most commonly used in management of anxiety disorders, specifically panic disorder or generalized anxiety disorder (GAD). Other uses include the treatment of chemotherapy-induced nausea, together with other treatments. GAD improvement occurs generally within a week. Alprazolam is generally taken by mouth.
Common side effects include sleepiness, depression or suppressed emotions, mild to severe decreases in motor skills, hiccups, dulling or declining of cognition as well as alertness or general awareness of one’s surroundings or even behavior, dry mouth (mildly), decreased heart rate, suppression (physiological inhibition) of general central nervous system activity (opposite of physiological excitation), impairment of judgment (usually in higher than therapeutic doses), marginal to severe decreases in memory formation, decreased ability to process new information, as well as partial to complete amnesia depending on dosage. Some of the sedation and tiredness may improve within a few days. Alprazolam withdrawal may occur if use is suddenly decreased; therefore, gradually decreasing the dosage over weeks or months may be required to mitigate the debilitating withdrawal symptoms or possible physical health complications of withdrawal. Alprazolam increases all-cause mortality.Cold turkey abstinence is therefore almost universally advised against for all benzodiazepines, with even tapering sometimes requiring attentive medical supervision and care. Alprazolam, like other benzodiazepines, acts through the GABAA receptor, which is considered to be the main mechanism of action responsible for its primary effects and its physiologically inhibiting components on the body’s central nervous system.
Alprazolam was invented by Jackson Hester at the Upjohn Company and patented in 1971 and approved for medical use in the United States in 1981. Alprazolam is a Schedule IV controlled substance and is a common drug of abuse. It is available as a generic medication. In 2020, it was the 37th most-commonly-prescribed medication in the United States, with more than 16 million prescriptions.
Medical uses


Alprazolam is mostly used in management of anxiety disorders, panic disorders, and nausea due to chemotherapy. Alprazolam is indicated for the treatment of generalized anxiety disorder and panic disorder with or without agoraphobia in adults. The FDA label advises that the physician should periodically reassess the usefulness of the drug.
Panic disorder
Alprazolam is effective in the relief of moderate to severe anxiety and panic attacks. Alprazolam is not recommended in Australia for the treatment of panic disorder because of concerns regarding tolerance, dependence, and abuse. Most evidence shows that the benefits of alprazolam in treating panic disorder last only four to ten weeks. However, people with panic disorder have been treated on an open basis for up to eight months without apparent loss of benefit.
Alprazolam is recommended by the World Federation of Societies of Biological Psychiatry (WFSBP) for treatment-resistant cases of panic disorder where there is no history of tolerance or dependence.
Anxiety disorders
Anxiety associated with depression is responsive to alprazolam. Clinical studies have shown that the effectiveness is limited to 4 months for anxiety disorders. However, the research into antidepressant properties of alprazolam is poor and has only assessed its short-term effects against depression. In one study, some long term, high-dosage users of alprazolam developed reversible depression. In the US, alprazolam is FDA-approved for the management of anxiety disorders (a condition corresponding most closely to the APA Diagnostic and Statistical Manual DSM-IV-TR diagnosis of generalized anxiety disorder) or the short-term relief of symptoms of anxiety. In the UK, alprazolam is recommended for the short-term treatment (2–4 weeks) of severe acute anxiety.
Nausea due to chemotherapy
Alprazolam may be used in combination with other medications for chemotherapy-induced nausea and vomiting.
Contraindications
Benzodiazepines require special precaution if used in children and in alcohol- or drug-dependent individuals. Particular care should be taken in pregnant or elderly people, people with substance use disorder history (particularly alcohol dependence), and people with comorbid psychiatric disorders. The use of alprazolam should be avoided or carefully monitored by medical professionals in individuals with: myasthenia gravis, acute narrow-angle glaucoma, severe liver deficiencies (e.g., cirrhosis), severe sleep apnea, pre-existing respiratory depression, marked neuromuscular respiratory, acute pulmonary insufficiency, chronic psychosis, hypersensitivity or allergy to alprazolam or other benzodiazepines, and borderline personality disorder (where it may induce suicidality and dyscontrol).
Like all central nervous system depressants, alprazolam in larger-than-normal doses can cause significant deterioration in alertness and increase drowsiness, especially in those unaccustomed to the drug's effects.
Elderly individuals should be cautious in the use of alprazolam due to the possibility of increased susceptibility to side-effects, especially loss of coordination and drowsiness.
Side effects

Sedative drugs, including alprazolam, have been associated with an increased risk of death.
Possible side effects include:
- Anterograde amnesia and concentration problems
- Ataxia, slurred speech
- Disinhibition
- Drowsiness, dizziness, lightheadedness, fatigue, unsteadiness, and impaired coordination, vertigo
- Dry mouth (infrequent)
- Hallucinations (rare)
- Jaundice (very rare)
- Seizures (less common)
- Skin rash, respiratory depression, constipation
- Suicidal ideation or suicide
- Urinary retention (infrequent)
- Muscle weakness
In September 2020, the U.S. Food and Drug Administration (FDA) required the boxed warning be updated for all benzodiazepine medicines to describe the risks of abuse, misuse, addiction, physical dependence, and withdrawal reactions consistently across all the medicines in the class.
Paradoxical reactions
Although unusual, the following paradoxical reactions have been shown to occur:
- Aggression
- Mania, agitation, hyperactivity, and restlessness
- Rage, hostility
- Twitches and tremor
Food and drug interactions
Alprazolam is primarily metabolized via CYP3A4. Combining CYP3A4 inhibitors such as cimetidine, erythromycin, norfluoxetine, fluvoxamine, itraconazole, ketoconazole, nefazodone, propoxyphene, and ritonavir delay the hepatic clearance of alprazolam, which may result in its accumulation and increased severity of its side effects.
Imipramine and desipramine have been reported to increase an average of 31% and 20% respectively by the concomitant administration of alprazolam tablets.Combined oral contraceptive pills reduce the clearance of alprazolam, which may lead to increased plasma levels of alprazolam and accumulation.
Alcohol is one of the most common interactions; alcohol and alprazolam taken in combination have a synergistic effect on one another, which can cause severe sedation, behavioral changes, and intoxication. The more alcohol and alprazolam taken, the worse the interaction. Combination of alprazolam with the herb kava can result in the development of a semi-comatose state. Plants in the genus Hypericum (including St. John's wort) conversely can lower the plasma levels of alprazolam and reduce its therapeutic effect.
Pregnancy and breastfeeding
Benzodiazepines cross the placenta, enter the fetus, and are also excreted in breast milk. Chronic administration of diazepam, another benzodiazepine, to nursing mothers has been reported to cause their infants to become lethargic and to lose weight.
The use of alprazolam during pregnancy is associated with congenital abnormalities, and use in the last trimester may cause fetal drug dependence and withdrawal symptoms in the post-natal period as well as neonatal flaccidity and respiratory problems. However, in long-term users of benzodiazepines, abrupt discontinuation due to concerns of teratogenesis has a high risk of causing extreme withdrawal symptoms and a severe rebound effect of the underlying mental health disorder. Spontaneous abortions may also result from abrupt withdrawal of psychotropic medications, including benzodiazepines.
Overdose

The maximum recommended daily dose is 10 milligrams per day.
Overdoses of alprazolam can be mild to severe depending on the quantity ingested and if other drugs are taken in combination.
Alprazolam overdoses cause excess central nervous system (CNS) depression and may include one or more of the following symptoms:
- Coma and death if alprazolam is combined with other substances.
- Fainting
- Hypotension (low blood pressure)
- Hypoventilation (shallow breathing)
- Impaired motor functions
- Dizziness
- Impaired balance
- Impaired or absent reflexes
- Muscle weakness
- Orthostatic hypotension (fainting while standing up too quickly)
- Somnolence (drowsiness)
Dependence and withdrawal
The potential for misuse among those taking it for medical reasons is controversial, with some expert reviews stating that the risk is low and similar to that of other benzodiazepine drugs. Others state that there is a substantial risk of misuse and dependence in both patients and non-medical users and that the short half-life and rapid onset of action may increase the risk of misuse. Compared to the large number of prescriptions, relatively few individuals increase their dose on their own initiative or engage in drug-seeking behavior.
Alprazolam, like other benzodiazepines, binds to specific sites on the GABAA (gamma-aminobutyric acid) receptor. When bound to these sites, which are referred to as benzodiazepine receptors, it modulates the effect of GABAA receptors and, thus, of GABAergic neurons. Long-term use causes adaptive changes in the benzodiazepine receptors, making them less sensitive to stimulation and thus making the drugs less potent.
Withdrawal and rebound symptoms commonly occur and necessitate a gradual reduction in dosage to minimize withdrawal effects when discontinuing.
Not all withdrawal effects are evidence of true dependence or withdrawal. Recurrence of symptoms such as anxiety may simply indicate that the drug was having its expected anti-anxiety effect and that, in the absence of the drug, the symptom has returned to pretreatment levels. If the symptoms are more severe or frequent, the person may be experiencing a rebound effect due to the removal of the drug. Either of these can occur without the person actually being drug dependent.
Alprazolam and other benzodiazepines may also cause the development of physical dependence, tolerance, and benzodiazepine withdrawal symptoms during rapid dose reduction or cessation of therapy after long-term treatment. There is a higher chance of withdrawal reactions if the drug is administered in a higher dosage than recommended, or if a person stops taking the medication altogether without slowly allowing the body to adjust to a lower-dosage regimen.
In 1992, Romach and colleagues reported that dose escalation is not a characteristic of long-term alprazolam users and that the majority of long-term alprazolam users change their initial pattern of regular use to one of symptom control only when required.
Some common symptoms of alprazolam discontinuation include malaise, weakness, insomnia, tachycardia, lightheadedness, and dizziness.
Those taking more than 4 mg per day have an increased potential for dependence. This medication may cause withdrawal symptoms upon abrupt withdrawal or rapid tapering, which in some cases have been known to cause seizures, as well as marked delirium similar to that produced by the anticholinergic tropane alkaloids of Datura (scopolamine and atropine). The discontinuation of this medication may also cause a reaction called rebound anxiety.
In a 1983 study, only 5% of patients who had abruptly stopped taking long-acting benzodiazepines after less than 8 months demonstrated withdrawal symptoms, but 43% of those who had been taking them for more than 8 months did. With alprazolam – a short-acting benzodiazepine – taken for 8 weeks, 65% of patients experienced significant rebound anxiety. To some degree, these older benzodiazepines are self-tapering.
The benzodiazepines diazepam and oxazepam have been found to produce fewer withdrawal reactions than alprazolam, temazepam, or lorazepam. Factors that determine the risk of psychological dependence or physical dependence and the severity of the benzodiazepine withdrawal symptoms during dose reduction of alprazolam include: dosage used, length of use, frequency of dosing, personality characteristics of the individual, previous use of cross-dependent/cross-tolerant drugs (alcohol or other sedative-hypnotic drugs), current use of cross-dependent/-tolerant drugs, use of other short-acting, high-potency benzodiazepines, and method of discontinuation.
Pharmacology

Alprazolam is a positive allosteric modulator of the gamma-aminobutyric acid (GABA) type A receptor. When it binds to the receptor, effects of GABA are enhanced leading to inhibition of neurons in the brain. This results in effects including reduced anxiety, muscle relaxant, antidepressant and anticonvulsant activity. The activity of alprazolam in the central nervous system is dose dependent.
Mechanism of action
Alprazolam is classed as a high-potency triazolobenzodiazepine: a benzodiazepine with a triazole ring attached to its structure. As a benzodiazepine, alprazolam produces a variety of therapeutic and adverse effects by binding to the GABAA benzodiazepine receptor site and modulating its function; GABA receptors are the most prolific inhibitory receptor within the brain. The GABA chemical and receptor system mediates inhibitory or calming effects of alprazolam on the nervous system. Binding of alprazolam to the GABAA receptor, a chloride ion channel, enhances the effects of GABA, a neurotransmitter. When GABA binds the GABAA receptor the channel opens and chloride enters the cell which makes it more resistant to depolarisation. Therefore, alprazolam has a depressant effect on synaptic transmission to reduce anxiety.
The GABAA receptor is made up of 5 subunits out of a possible 19, and GABAA receptors made up of different combinations of subunits have different properties, different locations within the brain, and, importantly, different activities with regard to benzodiazepines. Alprazolam and other triazolobenzodiazepines such as triazolam that have a triazole ring fused to their diazepine ring appear to have antidepressant properties. This is perhaps due to the similarities shared with tricyclic antidepressants, as they have two benzene rings fused to a diazepine ring. Alprazolam causes a marked suppression of the hypothalamic–pituitary–adrenal axis. The therapeutic properties of alprazolam are similar to other benzodiazepines and include anxiolytic, anticonvulsant, muscle relaxant, hypnotic and amnesic; however, it is used mainly as an anxiolytic.
Giving alprazolam, as compared to lorazepam, has been demonstrated to elicit a statistically significant increase in extracellular dopamine D1 and D2 concentrations in the striatum.
Pharmacokinetics
Alprazolam is taken orally, and is absorbed well – 80% of alprazolam binds to proteins in the serum (the majority binding to albumin). The concentration of alprazolam peaks after one to two hours.
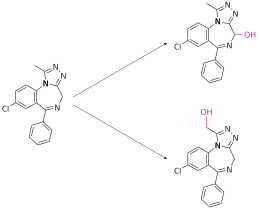
Alprazolam is metabolized in the liver, mostly by the enzyme cytochrome P450 3A4 (CYP3A4). Two major metabolites are produced: 4-hydroxyalprazolam and α-hydroxyalprazolam, as well as an inactive benzophenone. The low concentrations and low potencies of 4-hydroxyalprazolam and α-hydroxyalprazolam indicate that they have little to no contribution to the effects of alprazolam.
The metabolites, as well as some unmetabolized alprazolam, are filtered out by the kidneys and are excreted in the urine.
Chemistry
Physical properties
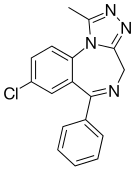
Alprazolam is a triazole and benzodiazepine derivative substituted with a phenyl group at position 6, with a chlorine atom at position 8 and with a methyl group at position 1. It is an analogue of triazolam, the difference between them being the absence of a chlorine atom in the ortho position of the phenyl ring. It is slightly soluble in chloroform, soluble in alcohol, slightly soluble in acetone and insoluble in water. It has a melting point of 228–229.5 °C (442.4–445.1 °F; 501.1–502.6 K).
Synthesis
For the synthesis of alprazolam the same method can be used as for triazolam, excepting that it starts from 2-amino-5-chlorobenzophenone. However, an alternative easier synthesis starting with 2,6-dichloro-4-phenylquinoline has been suggested, in which it reacts with hydrazine giving 6-chloro-2-hydrazino-4-phenylquinoline. Boiling the mixture with triethyl orthoacetate results in cyclization with the formation of the triazole ring. The product undergoes oxidative degradation in the presence of periodate and ruthenium dioxide in acetone solution, giving 2-[4-(3'-methyl-1,2,4-triazolo)]-5-chlorobenzophenone. Oxy-methylation with formaldehyde results in a product that is treated with phosphorus tribromide, when 2-[4-(3'-methyl-5'-bromomethyl-1,2,4-triazolo)]-5-chlorobenzophenone is obtained. By substituting the bromine atom with an amino group conferred by ammonia, it forms alprazolam triazolobenzophenone, following which an intermolecular heterocyclization takes place to obtain alprazolam.
Detection
Quantification of alprazolam in blood and plasma samples may be necessary to confirm a diagnosis of intoxication in hospitalized patients, or to provide evidence in the case of crimes e.g., impaired driving arrest, or to assist in a thorough forensic investigation, e.g., in a medicolegal death investigation. Blood or plasma alprazolam concentrations are usually in a range of 10–100 μg/L in persons receiving the drug therapeutically, 100–300 μg/L in those arrested for impaired driving, and 300–2,000 μg/L in victims of acute overdosage. Most of the commercial immunoassays used for the benzodiazepine class of drugs cross-react with alprazolam, but confirmation and quantitative determination are usually done by chromatographic techniques.
Forms of alprazolam
Alprazolam regular release and orally disintegrating tablets are available as 0.25 mg, 0.5 mg, 1 mg, and 2 mg tablets, while extended release tablets are available as 0.5 mg, 1 mg, 2 mg, and 3 mg. Liquid alprazolam is available in a 1 mg/mL oral concentrate. Inactive ingredients in alprazolam tablets and solutions include microcrystalline cellulose, corn starch, docusate sodium, povidone, sodium starch glycolate, lactose monohydrate, magnesium stearate, colloidal silicon dioxide, and sodium benzoate. In addition, the 0.25 mg tablet contains D&C Yellow No. 10 and the 0.5 mg tablet contains FD&C Yellow No. 6 and D&C Yellow No. 10.
Society and culture
Patent
Alprazolam is covered under U.S. Patent 3,987,052, which was filed on 29 October 1969, granted on 19 October 1976, and expired in September 1993.
Recreational use
There is a risk of misuse and dependence in both patients and non-medical users of alprazolam; alprazolam's high affinity binding, high potency, and rapid onset increase its abuse potential. The physical dependence and withdrawal syndrome of alprazolam also add to its addictive nature. In the small subgroup of individuals who escalate their doses there is usually a history of alcohol or other substance use disorders. Despite this, most prescribed alprazolam users do not use their medication recreationally, and the long-term use of benzodiazepines does not generally correlate with the need for dose escalation. However, based on US findings from the Treatment Episode Data Set (TEDS), an annual compilation of patient characteristics in substance abuse treatment facilities in the United States, admissions due to "primary tranquilizer" (including, but not limited to, benzodiazepine-type) drug use increased 79% from 1992 to 2002, suggesting that misuse of benzodiazepines may be on the rise. In 2011, The New York Times reported, "The Centers for Disease Control and Prevention last year reported an 89 percent increase in emergency room visits nationwide related to nonmedical benzodiazepine use between 2004 and 2008."
Alprazolam is one of the most commonly prescribed and misused benzodiazepines in the United States. A large-scale nationwide U.S. government study conducted by SAMHSA found that, in the U.S., benzodiazepines are recreationally the most frequently used pharmaceuticals due to their widespread availability, accounting for 35% of all drug-related visits to hospital emergency and urgent care facilities. Men and women are equally likely to use benzodiazepines recreationally. The report found that alprazolam is the most common benzodiazepine for recreational use, followed by clonazepam, lorazepam, and diazepam. The number of emergency department visits due to benzodiazepines increased by 36% between 2004 and 2006.
Regarding the significant increases detected, it is worthwhile to consider that the number of pharmaceuticals dispensed for legitimate therapeutic uses may be increasing over time, and DAWN estimates are not adjusted to take such increases into account. Nor do DAWN estimates take into account the increases in the population or in ED use between 2004 and 2006.
Those at a particularly high risk for misuse and dependence are people with a history of alcoholism or drug abuse and/or dependence and people with borderline personality disorder.
Alprazolam, along with other benzodiazepines, is often used with other recreational drugs. These uses include aids to relieve the panic or distress of dysphoric ("bad trip") reactions to psychedelic drugs, such as LSD, and the drug-induced agitation and insomnia in the "comedown" stages of stimulant use, such as amphetamine, cocaine, and MDMA allowing sleep. Alprazolam may also be used with other depressant drugs, such as ethanol, heroin, and other opioids, in an attempt to enhance their psychological effects. Alprazolam may be used in conjunction with cannabis, with users citing a synergistic effect achieved after consuming the combination.
The poly-drug use of powerful depressant drugs poses the highest level of health concerns due to a significant increase in the likelihood of experiencing an overdose, which may cause fatal respiratory depression.
A 1990 study found that diazepam has a higher misuse potential relative to many other benzodiazepines and that some data suggest that alprazolam and lorazepam resemble diazepam in this respect.
Anecdotally, injection of alprazolam has been reported, causing dangerous damage to blood vessels, closure of blood vessels (embolization) and decay of muscle tissue (rhabdomyolysis). Alprazolam is not very soluble in water—when crushed in water it does not fully dissolve (40 µg/ml of H2O at pH 7). There are also reports of alprazolam being snorted. Due to the low weight of a dose, alprazolam, in one case, was distributed on blotter paper in a manner similar to LSD.
Misuse of alprazolam and other benzodiazepines has been shown to cause cognitive impairment. Alprazolam has typically caused anterograde amnesia effects (inability to recall new events), but a study conducted on mice by the Department of Pharmaceutical Sciences and Drug Research at Punjabi University has also determined that Alprazolam can produce retrograde amnesic effects (inability to remember events occurring before amnesia).
Additionally, studies on the long-term cognitive effects of benzodiazepines found that long-term users of benzodiazepines still displayed cognitive deficits after 6 months of abstinence from constant usage.
Popular culture
Slang terms for alprazolam vary from place to place. Some of the more common terms are modified versions of the trade name "Xanax", such as Xannies (or Xanies) and the phonetic equivalent of Zannies; references to their drug classes, such as benzos or downers; or remark upon their shape or color (most commonly a straight, perforated tablet or an oval-shaped pill): bars, ladders, Xanbars, Xans, Z-bars, handle bars, beans, footballs, planks, poles, sticks, blues, or blue footballs.
The film "Take Your Pills: Xanax" (2022) gives the drug's history and usage.
Availability
Alprazolam is available in English-speaking countries under the following brand names:
- Alprax, Alprocontin, Alzam, Alzolam, Anzilum, Apo-Alpraz, Helex, Kalma, Mylan-Alprazolam, Niravam, Novo-Alprazol, Nu-Alpraz, Pacyl, Restyl, Tranax, Trika, Xycalm, Xanax, Xanor, Zolam, Zopax.
In December 2013, in anticipation of the rescheduling of alprazolam to Schedule 8 in Australia, Pfizer Australia announced they would be discontinuing the Xanax brand in Australia as it was no longer commercially viable.
Legal status
Alprazolam has varied legal status depending on jurisdiction:
- In the United States, alprazolam is a prescription drug and is assigned to Schedule IV of the Controlled Substances Act by the Drug Enforcement Administration.
- Under the UK drug misuse classification system, benzodiazepines are Class C drugs (Schedule 4). In the UK, alprazolam is not available on the NHS and can only be obtained on a private prescription.
- In Ireland, alprazolam is a Schedule 4 medicine.
- In Sweden, alprazolam is a prescription drug in List IV (Schedule 4) under the Narcotics Drugs Act (1968).
- In the Netherlands, alprazolam is a List 2 substance of the Opium Law and is available for prescription.
- In Germany, alprazolam can be prescribed normally in doses up to 1 mg. Higher doses are scheduled as Anlage III drugs and require a special prescription form.
- In Australia, alprazolam was originally a Schedule 4 (Prescription Only) medication; however, as of February 2014, it has become a Schedule 8 medication, subjecting it to more rigorous prescribing requirements.
- In the Philippines, alprazolam is legally classified as a "dangerous drug" under the Comprehensive Dangerous Drugs Act of 2002, along with other schedule drugs listed in the 1971 Convention on Psychotropic Substances. The importation of dangerous drugs including alprazolam, requires authorization from the Philippine Drug Enforcement Agency.
Internationally, alprazolam is included under the United Nations Convention on Psychotropic Substances as Schedule IV.
External links
- "Alprazolam". Drug Information Portal. U.S. National Library of Medicine.