
| Eardrum | |
|---|---|
 | |
 Right eardrum as seen through a speculum.
| |
| Details | |
| Identifiers | |
| Latin | membrana tympanica; myringa |
| MeSH | D014432 |
| TA98 | A15.3.01.052 |
| TA2 | 6870 |
| FMA | 9595 |
| Anatomical terminology | |
 |
| This article is one of a series documenting the anatomy of the |
| Human ear |
|---|
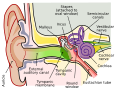
In the anatomy of humans and various other tetrapods, the eardrum, also called the tympanic membrane or myringa, is a thin, cone-shaped membrane that separates the external ear from the middle ear. Its function is to transmit sound from the air to the ossicles inside the middle ear, and then to the oval window in the fluid-filled cochlea. Hence, it ultimately converts and amplifies vibration in the air to vibration in cochlear fluid. The malleus bone bridges the gap between the eardrum and the other ossicles.
Rupture or perforation of the eardrum can lead to conductive hearing loss. Collapse or retraction of the eardrum can cause conductive hearing loss or cholesteatoma.
Structure
Orientation and relations
The tympanic membrane is oriented obliquely in the anteroposterior, mediolateral, and superoinferior planes. Consequently, its superoposterior end lies lateral to its anteroinferior end.
Anatomically, it relates superiorly to the middle cranial fossa, posteriorly to the ossicles and facial nerve, inferiorly to the parotid gland, and anteriorly to the temporomandibular joint.
Regions
The eardrum is divided into two general regions: the pars flaccida and the pars tensa. The relatively fragile pars flaccida lies above the lateral process of the malleus between the notch of Rivinus and the anterior and posterior malleal folds. Consisting of two layers and appearing slightly pinkish in hue, it is associated withEustachian tube dysfunction and cholesteatomas.
The larger pars tensa consists of three layers: skin, fibrous tissue, and mucosa. Its thick periphery forms a fibrocartilaginous ring called the annulus tympanicus or Gerlach's ligament. while the central umbo tents inward at the level of the tip of malleus. The middle fibrous layer, containing radial, circular, and parabolic fibers, encloses the handle of malleus. Though comparatively robust, the pars tensa is the region more commonly associated with perforations.
Umbo
The manubrium (Latin: handle) of the malleus is firmly attached to the medial surface of the membrane as far as its center, drawing it toward the tympanic cavity. The lateral surface of the membrane is thus concave. The most depressed aspect of this concavity is termed the umbo (Latin: shield boss).
Nerve supply
Sensation of the outer surface of the tympanic membrane is supplied mainly by the auriculotemporal nerve, a branch of the mandibular nerve (cranial nerve V3), with contributions from the auricular branch of the vagus nerve (cranial nerve X), the facial nerve (cranial nerve VII), and possibly the glossopharyngeal nerve (cranial nerve IX). The inner surface of the tympanic membrane is innervated by the glossopharyngeal nerve.
Clinical significance
Examination
When the eardrum is illuminated during a medical examination, a cone of light radiates from the tip of the malleus to the periphery in the anteroinferior quadrant, this is what is known clinically as 5 o'clock.
Rupture
Unintentional perforation (rupture) has been described in blast injuries and air travel, typically in patients experiencing upper respiratory congestion that prevents equalization of pressure in the middle ear. It is also known to occur in swimming, diving (including scuba diving), and martial arts.
Patients with tympanic membrane rupture may experience bleeding, tinnitus, hearing loss, or disequilibrium (vertigo). However, they rarely require medical intervention, as between 80 and 95 percent of ruptures recover completely within two to four weeks. The prognosis becomes more guarded as the force of injury increases.
Surgical puncture for treatment of middle ear infections
The pressure of fluid in an infected middle ear onto the eardrum may cause it to rupture. Usually, this consists of a small hole (perforation), which allows fluid to drain out. If this does not occur naturally, a myringotomy (tympanotomy, tympanostomy) can be performed. A myringotomy is a surgical procedure in which a tiny incision is created in the eardrum to relieve pressure caused by excessive buildup of fluid, or to drain pus from the middle ear. The fluid or pus comes from a middle ear infection (otitis media), which is a common problem in children. A tympanostomy tube is inserted into the eardrum to keep the middle ear aerated for a prolonged time and to prevent reaccumulation of fluid. Without the insertion of a tube, the incision usually heals spontaneously in two to three weeks. Depending on the type, the tube is either naturally extruded in 6 to 12 months or removed during a minor procedure.
Those requiring myringotomy usually have an obstructed or dysfunctional eustachian tube that is unable to perform drainage or ventilation in its usual fashion. Before the invention of antibiotics, myringotomy without tube placement was also used as a major treatment of severe acute otitis media.
In some cases, the pressure of fluid in an infected middle ear is great enough to cause the eardrum to rupture naturally. Usually, this consists of a small hole (perforation), from which fluid can drain.
Society and culture
The Bajau people of the Pacific intentionally rupture their eardrums at an early age to facilitate diving and hunting at sea. Many older Bajau therefore have difficulties hearing.
See also
- Middle ear
- Valsalva maneuver to equalize pressure across the eardrum
Additional images

External and middle ear, right side, opened from the front (coronal section)

Horizontal section through left ear; upper half of section

The right membrana tympani with the hammer and the chorda tympani, viewed from within, from behind, and from above

Auditory tube, laid open by a cut in its long axis
![Chain of ossicles and their ligaments, seen from the front in a vertical, transverse section of the tympanum [tympanic cavity]](//upload.wikimedia.org/wikipedia/commons/thumb/5/5f/Gray919.png/82px-Gray919.png)
Chain of ossicles and their ligaments, seen from the front in a vertical, transverse section of the tympanum [tympanic cavity]

Right eardrum as seen through a speculum

This is a normal left eardrum.

Tympanic membrane viewed by otoscope

The oval perforation in this left tympanic membrane was the result of a slap on the ear

A subtotal perforation of the right tympanic membrane resulting from a previous severe otitis media

A normal human right tympanic membrane (eardrum)

Frog on leaf showing eardrum





![Chain of ossicles and their ligaments, seen from the front in a vertical, transverse section of the tympanum [tympanic cavity]](http://upload.wikimedia.org/wikipedia/commons/thumb/5/5f/Gray919.png/82px-Gray919.png)







![]() This article incorporates text in the public domain from page 1039 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 1039 of the 20th edition of Gray's Anatomy (1918)