
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Numorphan, Numorphone, Opana, others |
| Other names | 14-Hydroxydihydromorphinone |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a610022 |
| License data |
|
| Routes of administration |
By mouth, buccal, sublingual, intranasal, intravenous, epidural, subcutaneous, intramuscular |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | by mouth: 10% Buccal: 28% Sublingual: 37.5% Intranasal: 43% IV, IM & IT: 100% |
| Protein binding | 10% |
| Metabolism | Liver (CYP3A4, glucuronidation) |
| Elimination half-life | 7–9 hours Duration of Action: 6-8 hours Orally, 4-6 hrs Parenteral. |
| Excretion | Urine, feces |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.000.873 |
| Chemical and physical data | |
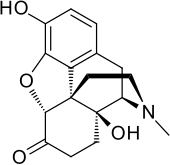
| Formula | C17H19NO4 |
| Molar mass | 301.342 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
| (verify) | |
Oxymorphone (sold under the brand names Numorphan and Opana among others) is a highly potent opioid analgesic indicated for treatment of severe pain. Pain relief after injection begins after about 5–10 minutes, after oral administration it begins after about 30 minutes, and lasts about 3–4 hours for immediate-release tablets and 12 hours for extended-release tablets. The elimination half-life of oxymorphone is much faster intravenously, and as such, the drug is most commonly used orally. Like oxycodone, which metabolizes to oxymorphone, oxymorphone has a high potential to be abused.
It was developed in Germany in 1914. It was patented in 1955 and approved for medical use in 1959. In June 2017 the FDA asked Endo Pharmaceuticals to remove its product from the US market. This was in part due to the opioid epidemic in the US, and the fact that a 2012 reformulation failed to stop illicit injection of the drug. Endo responded by voluntarily removing Opana ER from the market a month later. Generic versions of extended-release oxymorphone, such as those manufactured by Amneal Pharmaceuticals, are still available in the US.
Medical uses
Oxymorphone Immediate Release is indicated for the relief of moderate to severe pain, such as treatment of acute post surgical pain. For any chronic treatment of pain, clinicians should only consider long term use if there is significant clinical benefit to the patient's therapy that outweigh any potential risk. The first line treatment choices for chronic pain are non-pharmacological and non-opioid agents.
Oxymorphone extended-release tablets are indicated for the management of chronic pain and only for people already on a regular schedule of strong opioids for a prolonged period. Immediate-release oxymorphone tablets are recommended for breakthrough pain for people on the extended-release version. Compared to other opioids, oxymorphone has similar pain relieving efficacy.
In the United States it is a Schedule II controlled substance with an ACSCN of 9652.
Oxymorphone ER Tablets should be taken on an empty stomach.
Availability
Brands and forms
Oxymorphone was marketed by Endo Pharmaceuticals, under the brand name(s) Opana and Opana ER. Opana ER was withdrawn by the manufacturer in 2017 due to a FDA request, making it unavailable in the US. However, both IR (immediate release) and ER (extended release) formulations are still available under the generic name Oxymorphone and Oxymorphone ER, provided by a multitude of different manufacturers.
Oxymorphone is also available as an injectable for inpatient use, available for IV (intravenous), IM (intramuscular), and SC (subcutaneous) injection.
An extended release (ER) modified-release dosage form is commonly used, which modifies the pharmacokinetics of the drug.
Oral dosage forms
Oxymorphone comes in a variety of doses.
| IR Tablet | ER 12 Hour Tablet |
|---|---|
| 5 mg | 5 mg |
| 10 mg | 7.5 mg |
| 10 mg | |
| 15 mg | |
| 20 mg | |
| 30 mg | |
| 40 mg |
Special populations
Patients already suffering from debilitation are at a much higher risk of respiratory depression. Nonopioid analgesics should be considered in this population.
Elderly patients are much more sensitive to adverse effects, such as falls, cognitive impairment and constipation, and should be monitored for such. Decreased renal function associated with aging leads to decreased clearance of the drug, resulting in narrow therapeutic windows and increasing the danger of overdose. If oxymorphone is absolutely indicated, smaller initial doses should be started for this population.
There is a risk of neonatal withdrawal symptom in the newborn if pregnant women take oxymorphone for a prolonged period. Oxymorphone crosses the placenta and holds risk of birth defects, poor fetal growth, stillbirth, and preterm delivery. The children of mothers who are physically dependent on oxymorphone have a higher risk of similar dependence. Due to these severe risks, oxymorphone is highly discouraged among this population. The amount of transfer of oxymorphone into the breast milk is not known and women are cautioned to weigh the risks and benefits before breastfeeding while on this medication.
Side effects
The principal adverse effects of oxymorphone are similar to other opioids with constipation, nausea, vomiting, dizziness, dry mouth and drowsiness being the most common adverse effects. This drug is highly addictive as with other opioids and can lead to chemical dependence and withdrawal.
Overdose
In common with other opioids, oxymorphone overdosage is characterized by respiratory depression, sleepiness progressing to stupor or coma, skeletal muscle weakness, cold and clammy skin, and sometimes slow heart rate and low blood pressure. In a severe case of overdose, apnea, circulatory collapse, cardiac arrest and death can occur.
Pharmacology
Pharmacodynamics
Oxymorphone elicits its effects by binding to and activating the μ-opioid receptor (MOR) and, to a much lesser extent, the δ-opioid receptor (DOR) and κ-opioid receptor (KOR). Its activity at the DOR may augment its action at the MOR. Oxymorphone is 10 times more potent than morphine. The calculation of relative potency indicated that 1 mg of oxymorphone hydrochloride equaled 9.85 mg of morphine sulfate, or 1.02 mg of oxymorphone hydrochloride was equivalent to 10 mg of morphine sulfate.
| Affinities (Ki) | Ratio | ||
|---|---|---|---|
| MOR | DOR | KOR | MOR:DOR:KOR |
| 0.78 nM | 50 nM | 137 nM | 1:64:176 |
| Compound | Route | Dose |
|---|---|---|
| Codeine | PO | 200 mg |
| Hydrocodone | PO | 20–30 mg |
| Hydromorphone | PO | 7.5 mg |
| Hydromorphone | IV | 1.5 mg |
| Morphine | PO | 30 mg |
| Oxycodone | IV | 20 mg |
| Morphine | IV | 10 mg |
| Oxycodone | PO | 20 mg |
| Oxymorphone | PO | 7–10 mg |
| Oxymorphone | IV | 1 mg |
Pharmacokinetics
Chemistry
Oxymorphone is commercially produced from thebaine, which is a minor constituent of the opium poppy (Papaver somniferum) but thebaine is found in greater abundance (3%) in the roots of the oriental poppy (Papaver orientale). German patents from the mid-1930s indicate that oxymorphone as well as hydromorphone, hydrocodone, oxycodone, and acetylmorphone can be prepared—without the need for hydrogen gas—from solutions of codeine, morphine, and dionine by refluxing an acidic aqueous solution, or the precursor drug dissolved in ethanol, in the presence of certain metals, namely palladium and platinum in fine powder or colloidal form or platinum black.
Oxymorphone hydrochloride occurs as odourless white crystals or white to off-white powder. It darkens in colour with prolonged exposure to light. One gram of oxymorphone hydrochloride is soluble in 4 ml of water and it is sparingly soluble in alcohol and ether. It degrades upon contact with light.
Oxymorphone can be acetylated like morphine, hydromorphone, and some other opioids. Mono-, di-, tri-, and tetra- esters of oxymorphone were developed in the 1930s but are not used in medicine at this time. Presumably other esters such as nicotinyl, benzoyl, formyl, cinnimoyl &c.can be produced.
The 2013 US DEA annual manufacturing quotas were 18 375 kilogrammes for conversion (a number of drugs can be made from oxymorphone, both painkillers and opioid antagonists like naloxone) and 6875 kg for direct manufacture of end-products. Oxymorphone is also a minor metabolite of oxycodone, which is formed by CYP2D6-mediated O-demethylation.
History
Oxymorphone was first developed in Germany in 1914, and patented in the US by Endo Pharmaceuticals in 1955. It was introduced in the United States in January 1959 and other countries around the same time.
Society and culture
Brand names
- Numorphan (suppository and injectable solution)
- Opana ER (extended-release tablet): June 2017 FDA removal request due to rates of IV abuse.
- Opana IR (immediate-release tablet)
- O-Morphon in Bangladesh by Ziska pharmaceutical ltd.
The brand name Numorphan is derived by analogy to the Nucodan name for an oxycodone product (or vice versa) as well as Paramorphan/Paramorfan for dihydromorphine and Paracodin (dihydrocodeine). The only commercially available salt of oxymorphone in most of the world at this time is the hydrochloride, which has a free base conversion ratio of 0.891, and oxymorphone hydrochloride monohydrate has a factor of 0.85.
Generic pill markings are ATV10/APO; HK10 (10 mgs) oblong white and ATV20/APO; HK20 (20 mgs) oblong white.
Abuse
In 1924, the United States Congress had banned the sale, importation, or manufacture of heroin, another opioid pain medication in the Anti-Heroin Act of 1924.
In the past 30 years, opioid drug abuse has been a prevalent public health issue. In more recent years, this issue has developed into a full-fledged epidemic and is leading to several other public health issues, including the spread of diseases like hepatitis C and human immunodeficiency virus (HIV).
In the United States, as of 2013 more than 12 million people abused opioid drugs at least once a year. In 2010, 16,652 deaths were related to opiate overdose, in 2015 this number increased to 33,091. In September 2013, new FDA labeling guidelines for long-acting and extended-release opioids required manufacturers to remove moderate pain as use indication, reserving the drug for "pain severe enough to require daily, around-the-clock, long-term opioid treatment" however it did not restrict physicians from prescribing opioids for moderate, "as needed" usage.
In January 2013, the Centers for Disease Control and Prevention (CDC) reported an illness associated with intravenous (IV) abuse of oral Opana ER (oxymorphone) in Tennessee. The syndrome resembled that of thrombotic thrombocytopenic purpura (TTP). Initial therapy included therapeutic plasma exchange, as for TTP. Unlike TTP, no deficient ADAMTS13 activity nor anti-ADAMTS13 antibody was found indicating a thrombotic microangiopathy of different underlying cause. If IV Opana abuse is acknowledged, supportive care, instead of therapeutic plasma exchange could be considered.
In January 2015, the first HIV outbreak linked to abuse of prescription opioid drugs was identified by the Indiana State Department of Health (ISDH), in the small, rural community of Scott County in southeastern Indiana. ISDH launched an investigation into this HIV outbreak when 11 individuals were confirmed positive for HIV with ties tracing back to the same community. Three months into this investigation, ISDH diagnosed a total of 135 people with HIV, with the numbers still increasing. The cause of this outbreak has been linked to the sharing of needles between opioid abusers, which in some cases, involves sharing needles with up to nine different partners.
In late March 2015, reports indicated Austin, Indiana, was the center of an outbreak of HIV caused by oxymorphone use as an injectable recreational drug. The outbreak required emergency action by state officials. The NPR podcast "embedded" episode of March 31, 2016 was an in-depth account of a visit to oxymorphone abusers in Austin, Indiana. In 2016, the street price of oxymorphone was reported to be $140.
The common opioid of abuse in this outbreak has been identified as Opana ER, a time-released oxymorphone pain killer formulated to be resistant to crushing, manufactured by Endo Pharmaceuticals. This harder to crush formulation was put into production in 2012 in an effort to reduce the risk of abuse from snorting the crushed up pill. However, opioid abusers circumvented this issue by finding a way to dissolve and inject the drug.
The extent of this outbreak has garnered the attention of both the CDC and FDA. The CDC opened a larger investigation into all disease outbreaks involving Opana ER, focusing on the incidence of thrombotic thrombocytopenic purpura (TTP)-like illness in the 2012 Tennessee outbreak, as well as the 2015 HIV outbreak in Indiana. The FDA launched a post-marketing safety study regarding the reformulation of Opana ER in 2012 and the Indiana state government helped fund another study exploring the link between HIV infection and injection use of oxymorphone in Indiana from 2014 to 2015.
The results of these studies found that the reformulation of Opana to a hard to crush tablet unintentionally increased the risk of transmission of acquired blood borne infections because opioid abusers switched from using the drug through the nasal route to injection. This epidemic caused the risk of acquiring a blood borne infection with the use of injectable opioids to increase in comparison to the risk of acquiring an infection when using injectable heroin or cocaine.
In June 2017, faced with the public health crisis, the opioid epidemic, the FDA asked Endo Pharmaceuticals to "remove its opioid pain medication, reformulated Opana ER (oxymorphone hydrochloride), from the market". In their June 8, 2017 press release they also noted that, this was the first time the FDA had taken steps to "remove a currently marketed opioid pain medication from sale due to public health consequences of abuse." By July 6, 2017, Endo International voluntarily complied with the FDA removal request.
See also
![]() Media related to Oxymorphone at Wikimedia Commons
Media related to Oxymorphone at Wikimedia Commons